In 2009, 3796 individuals in Canada were placed on the wait list to receive an organ transplant (CIHI, 2009). Of those 3796 people, only 2155 transplants were performed and 249 people died waiting for their vital organ (CIHI, 2009). These statistics do not include the thousands of people who did not qualify for organ transplantation but still required life saving intervention. It is unlikely that the future will bring any substantial increases in the number of transplants preformed due to the availability of organs. Clearly alternative therapeutic options must be developed and utilized. The use of mechanical organs is one viable option.
The idea of mechanical or artificial organs has been around for centuries. During the 17th century, English scientist and philosopher Robert Hooke first conceptualized the idea of an artificial device substituting an organ (Lim, 2006). The exploration of mechanical devices remained merely experimental until the 20th century when the advancement of biomedical knowledge rapidly increased and the success of replacing and supplementing human functions occurred. Substantial research and innovation has occurred since Hooke’s time and we will focus on the history and pathophysiology of the mechanical lung, heart and kidney.
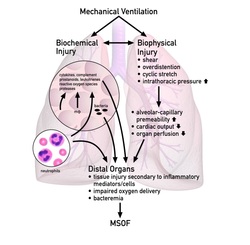
The artificial lung or oxygenators have been used during surgery, for emergency support, as a bridge to transplantation and most recently as a true replacement of the lung in the form of an implantable device. Hooke was able to demonstrate, experimentally in 1665, that inflation and deflation of the lungs was not compulsory for the oxygenation of blood flowing through them (Lim, 2006). In 1939, J. Gibbon first used an artificial lung and it remained a tool used by researchers, due to its complexity and difficulty to use by all it was not utilized commercially (Nogawa, 2002). In 1970, the artificial lung was transformed from research project to commercial product. The disposable bubble oxygenator became reliable and available internationally in the 1980’s but it was termed an oxygenator instead of an artificial lung since it was approved for short term use only (Nogawa, 2002). Due to our current crisis related to the shortage of donor organs and a steady increase in need, there is a push to develop an implantable artificial lung that would truly serve as a bridge to transplant. Mechanical ventilators are unable to replace the function of the lung without sedation, risk of injury and negative outcomes.
The idea of mechanical or artificial organs has been around for centuries. During the 17th century, English scientist and philosopher Robert Hooke first conceptualized the idea of an artificial device substituting an organ (Lim, 2006). The exploration of mechanical devices remained merely experimental until the 20th century when the advancement of biomedical knowledge rapidly increased and the success of replacing and supplementing human functions occurred. Substantial research and innovation has occurred since Hooke’s time and we will focus on the history and pathophysiology of the mechanical lung, heart and kidney.
The artificial lung or oxygenators have been used during surgery, for emergency support, as a bridge to transplantation and most recently as a true replacement of the lung in the form of an implantable device. Hooke was able to demonstrate, experimentally in 1665, that inflation and deflation of the lungs was not compulsory for the oxygenation of blood flowing through them (Lim, 2006). In 1939, J. Gibbon first used an artificial lung and it remained a tool used by researchers, due to its complexity and difficulty to use by all it was not utilized commercially (Nogawa, 2002). In 1970, the artificial lung was transformed from research project to commercial product. The disposable bubble oxygenator became reliable and available internationally in the 1980’s but it was termed an oxygenator instead of an artificial lung since it was approved for short term use only (Nogawa, 2002). Due to our current crisis related to the shortage of donor organs and a steady increase in need, there is a push to develop an implantable artificial lung that would truly serve as a bridge to transplant. Mechanical ventilators are unable to replace the function of the lung without sedation, risk of injury and negative outcomes.
BioLung

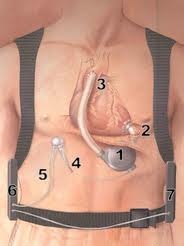
Today there is a thoracic artificial lung which has hope of becoming a life saver to those awaiting lung transplants. The BioLung is a device that is implanted in the thoracic cavity and is no larger than a soda can (Sato et al., 2007). It uses the person’s own heart, not a mechanical pump, to pump blood into the device which manages oxygen and blood flow throughout the body.
This is a step towards creating a long term replacement of a human lung and is freeing people from heavy life sustaining equipment
This is a step towards creating a long term replacement of a human lung and is freeing people from heavy life sustaining equipment
VAD
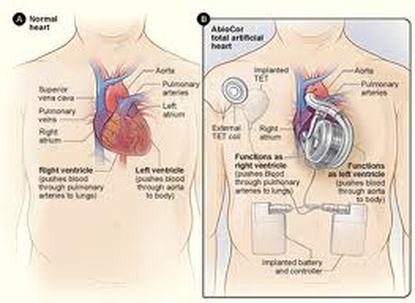
The early researches into mechanical circulatory systems were not intended as a replacement of the heart. Studies dating back to as early as 1885 document artificial heart-lung apparatuses being built in order to study organ perfusion (ASAIO, 2010). This work led to the use of heart-lung machines for cardiac surgeries. After the first heart transplant in 1963, work began to develop an implantable artificial heart (Roth & Lenfant, 1990). Since then many devices have been created to allow patients with end stage heart disease survive until a suitable donor was found. One such device is the ventricular assist device (VAD).
It is not a replacement for the heart but a device that assists the heart to function. In 2001, Robert Tools was the first person to successfully receive a total artificial heart transplant (TAH) (Simmons, 2001). Mr. Tools was not a candidate for transplant and his was death imminent. The TAH allowed for increased function of his other vital organs which in turn prolonged his life.
It is not a replacement for the heart but a device that assists the heart to function. In 2001, Robert Tools was the first person to successfully receive a total artificial heart transplant (TAH) (Simmons, 2001). Mr. Tools was not a candidate for transplant and his was death imminent. The TAH allowed for increased function of his other vital organs which in turn prolonged his life.
It is not a replacement for the heart but a device that assists the heart to function. In 2001, Robert Tools was the first person to successfully receive a total artificial heart transplant (TAH) (Simmons, 2001). Mr. Tools was not a candidate for transplant and his was death imminent. The TAH allowed for increased function of his other vital organs which in turn prolonged his life.